Anatomy map
Danger Map
Click me
Beware the 3 danger points
Click Stress Points to cycle through cleared-root examples where sharp curves, hooks, and wall contact bind, fatigue, and break files if the anatomy is not controlled.
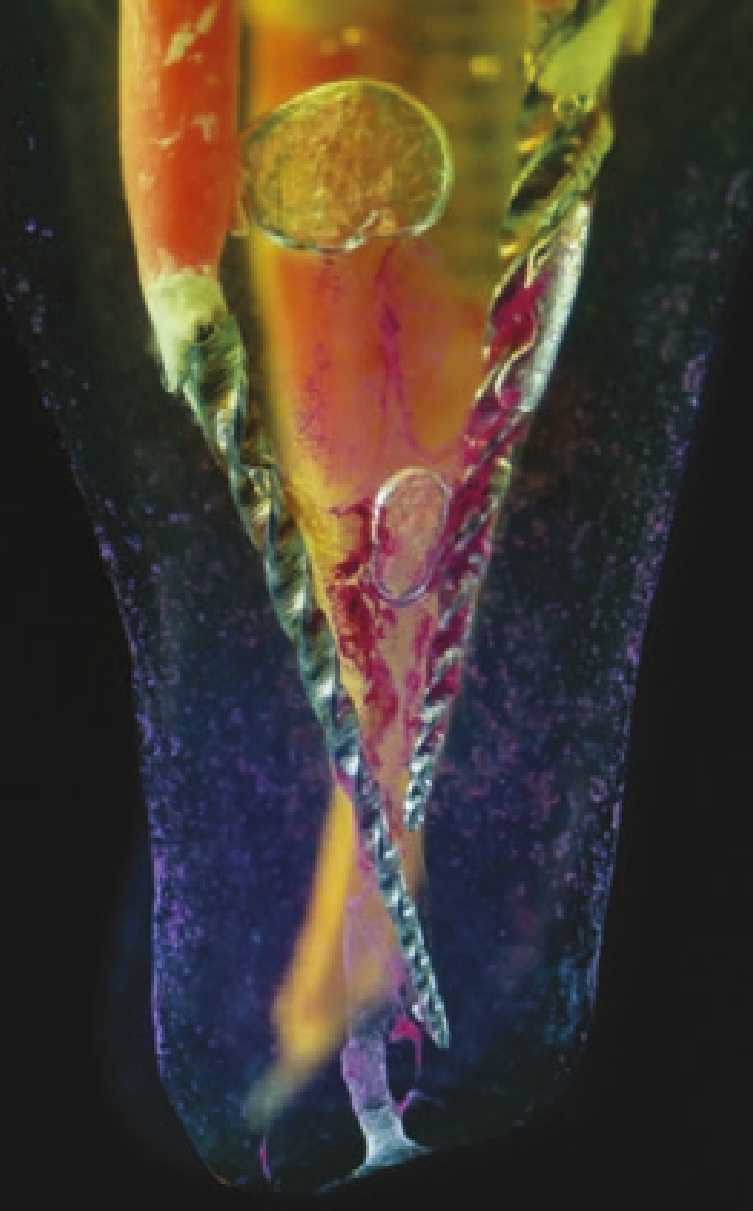
Mesial root stress point
A cleared lower molar root showing why curvature must be read before shaping pressure is added.